






| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 1, Number 4-5, October 2012, pages 118-120
A Locally Advanced Squamous Cell Carcinoma of the Ureter
Omer A Raheema, b, Emam Elmusharafa, Rowan G Caseya, Ted McDermotta
aDepartment of Urology, St James’s hospital, Dublin, Ireland
bCorresponding author: Omer A Raheem, Registrar in Urology, Department of Urology, St James’s hospital, James’s street, Dublin 8, Ireland
Manuscript accepted for publication October 3, 2012
Short title: Squamous Cell Carcinoma of the Ureter
doi: https://doi.org/10.4021/wjnu53w
| Abstract | ▴Top |
Squamous cell carcinoma of the ureter is very rare, constituting only 1-1.6% of all urothelial tumours. It is an aggressive tumor, spreading to bone, liver and lung. The median post diagnosis survival is short and estimated to be five months. Definitive diagnosis is exclusively by histology. Therapeutic options may include radical surgery, radiotherapy, chemotherapy, or a combination of these treatments. We present a case of locally advanced squamous cell carcinoma of the ureter and comment on its clinical management and subsequent oncological outcomes.
Keywords: Ureter; Squamous cell; Carcinoma
| Introduction | ▴Top |
The vast majority of the upper urinary tract carcinomas, including the renal pelvis and ureter are urothelial in origin [1]. Although rare, squamous cell carcinoma (SCC) of the upper urinary tracts does exist and constitutes only 1-1.6% of all urothelial carcinomas. Adding to its rarity, the occurrence of the SCC in the renal pelvis is approximately six times higher, compared to the ureter [1]. Patients usually present in their sixth and seven decade.
Numerous risk factors have been previously postulated to play major role in the development of the SCC of the ureter such as chronic irritation, urolithiasis, chronic hydronephrosis, heavy misuse of analgesics especially Phenacetin and external beam irradiation [1, 2]. In addition to the abovementioned risk factors, horse-shoe kidneys have a higher tendency to develop SCC of the uerter than normal kidney [2]. The ueteric mucosa is transitional in origin and normally lacks squamous architecture. Hence the tumorigenesis of the SCC of the ureter can be partly explained by the chronic irritation leading to de-differentiation, dysplasia and ultimately SCC [2].
Therapeutic options may include radical surgery, radiotherapy, chemotherapy, or a combination of these treatments. We present a case of locally advanced SCC of the ureter and comment on its management and subsequent disease related complication.
| Case Report | ▴Top |
A 57-years-old caucasian male presented to the university hospital with gross painless hematuria for three days duration. Patients denied history of abdominal pain or weight loss. Previous past medical history of gallstones pancreatitis managed conservatively. No previous hazardous occupational exposures or smoking history. Clinical examination was unremarkable. Haematological and biochemical profile was within normal ranges. Hemoglobin level was 13.3 g/L (normal range 13.5 - 18 g/dL), creatinine was 100 µmol/L (normal range 62 - 106 µmol/L) and serum amylase was 42 mg/dL (20 - 92 mg/dL). Urinalysis and urine cytology were normal and negative for the presence of malignant urothelial cells.
On contrast Computerized Tomography (CT) of the abdomen and pelvis showed a filling defect on the upper third of left ureter just below uretero-pelvic junction (UPJ) with proximal ureteric dilatation concerning for ureteric carcinoma (Fig. 1A, B ). No evidence of distant metastasis was found. To further delineate the ureteric filling defect, flexible ureteroscopy and retrograde study was subsequently performed and revealed a filling defect below the left UPJ (Fig. 1C). This lesion was directly visualized by flexible ureteroscope and revealed 2 cm polypoid like tumour just below the left UPJ. Direct biopsy and/or brush cytology of this tumour was failed due to its excessive mobility of the lesion.
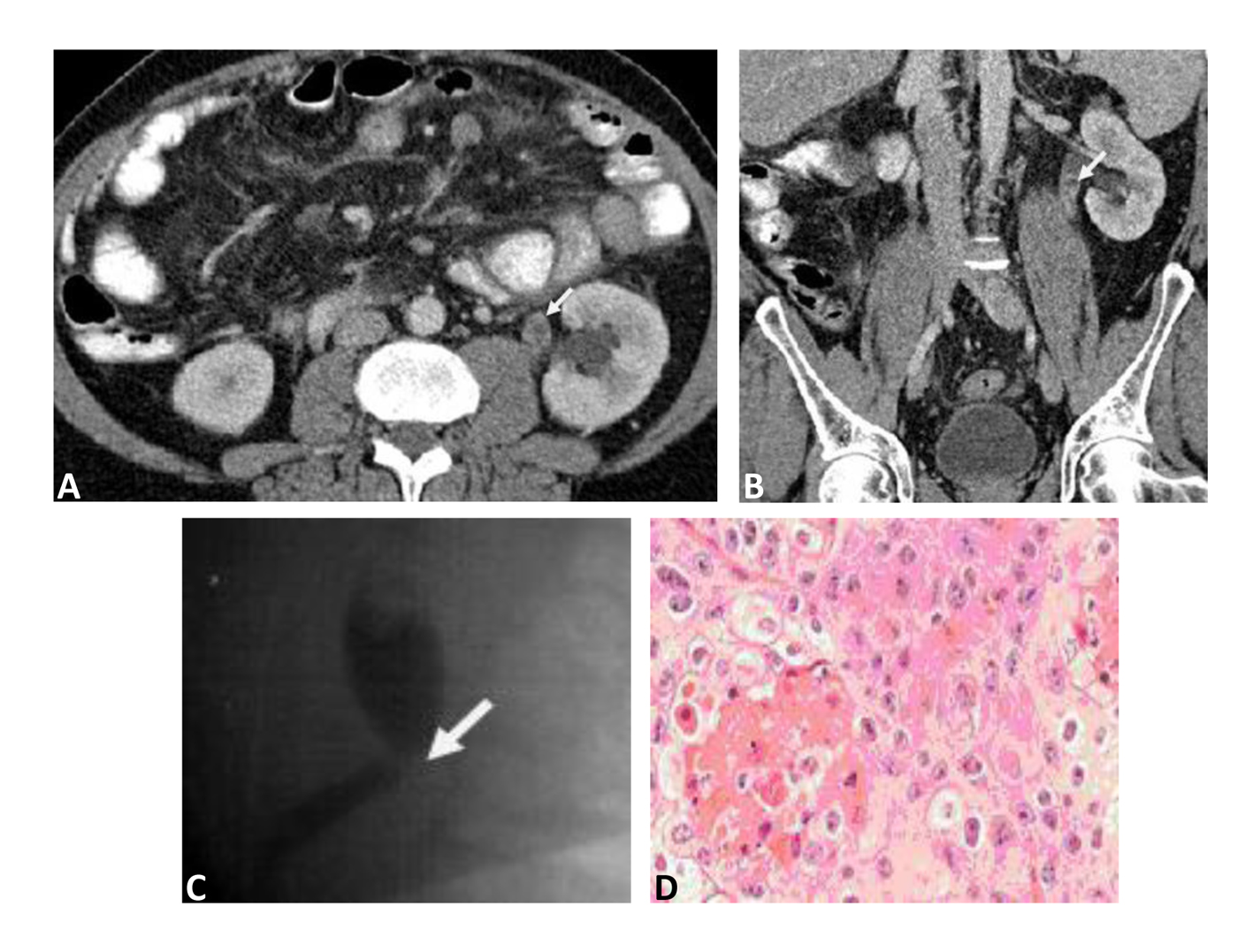 Click for large image | Figure 1. A: Transverse section Contrast Computerized Tomography (CT) image, a filling defect is demonstrated in the left upper ureter (just below the uretero-pelvic junction) (marked by white arrow). B: Sagittal section Contrast Computerized Tomography (CT) image, a filling defect is demonstrated in the left upper ureter (just below the uretero-pelvic junction) (marked by white arrow). C: Retrograde contrast study of left ureter, a filing defect is shown just below the uretero-pelvic junction (marked by white arrow). D: A high power (20 × objectives) of squamous cell carcinoma of the left ureter, nests of squamous cells with hyperchromatic nuclei and prominent keratin production (Haematoxylin and Eosin stain). |
After multidisciplinary team meeting and thorough discussion with the patient in regards to the therapeutics modalities available. This patient opted to undergo an open left radical nephro-ureterectomy which was subsequently performed successfully. Histology of the specimen showed urothelial solid tumour 18 × 10 mm with squamous differentiation. No involvement of lamina properia (pT1N0M0) or vascular/lymphatic invasions (Fig. 1D). Post operatively, the patient made an uncomplicated recovery and subsequently discharged home. On his first 3-monthly follow-up visit, patient was clinically well and all his abdominal wounds have healed. To date, cystoscopical examination of patient’s urinary bladder showed also no evidence of tumour recurrence. In addition, CT follow-up revealed no evidence of local recurrence or distant metastasis.
| Discussion | ▴Top |
Although, the vast majority of the ureteric carcinomas are urothelial in origin, SCC of the upper urinary tracts is very rare and constitutes only 1-1.6% of all urothelial carcinomas [1, 2]. The common age of presentation is the 6th decade of life. Patients with SCC of the ureter may present with local symptoms like loin discomfort or pain. These symptoms can be due to mechanical obstruction of the ureter, leading to hydonephrosis and renal capsular stretching [3]. Hematuria is another common clinical presentation which needs thorough investigations. Additionally, para-neoplastic syndromes can also manifest, and cause hypercalcemia, leucocytosis and thrombocytopenia [1]. Distant metastasis of the SCC of the ureter can also occur in lymph nodes, skin, lungs, liver and bone [4]. The median post diagnosis survival is short and estimated to be five months. The definitive diagnosis is confirmed by the presence of histological features of SCC differentiation such as squamous de-differentiation and keratin pearls.
Several therapeutic approaches have been employed in the management of the SCC of the ureter, including radical surgery, neo-adjuvant and/or adjuvant radiotherapy and chemotherapy. However, published data of these therapeutics modalities have shown limited survival benefit [1]. Radical surgery such as radical nephro-ureterctomy is considered to be the main therapeutic modality for SCC of the ureter [2]. Prognosis is very poor and invariably depends on staging and grading of the SCC of the ureter at the time of diagnosis. Due to the aggressiveness of the SCC of the ureter, patients often present with late stage T3 disease. Overall 5-years survival rate is very less than 10%. If diagnosed early, SCC of the ureter can be successfully managed by radical surgery. The lack of large randomized trials can be partly explained by the rarity of the diagnosis, the locally advanced nature of the disease, with rapid disease progression in many patients, thus limiting the opportunity to determine more effective treatment options for these patients.
In addition, SCC of the ureter carries dismal prognosis because of its late presentation. There is limited reported benefit from radio-chemotherapy in this setting. This case highlights an early and radical management of ureteric SCC with desirable oncological outcomes.
In conclusion, squamous cell carcinoma of the ureter is very rare, constituting only 1-1.6% of all urothelial tumours. It is an aggressive tumor, spreading to bone, liver and lung. The median post diagnosis survival is short and estimated to be five months. Definitive diagnosis is exclusively by histology. Therapeutic options may include radical surgery, radiotherapy, chemotherapy, or a combination of these treatments. We present a case of locally advanced squamous cell carcinoma of the ureter and comment on its clinical management and subsequent oncological outcomes.
| References | ▴Top |
- Busby JE, Brown GA, Tamboli P, Kamat AM, Dinney CP, Grossman HB, Matin SF. Upper urinary tract tumors with nontransitional histology: a single-center experience. Urology. 2006;67(3):518-523.
doi pubmed - Holmang S, Lele SM, Johansson SL. Squamous cell carcinoma of the renal pelvis and ureter: incidence, symptoms, treatment and outcome. J Urol. 2007;178(1):51-56.
doi pubmed - Toktas G, Ergun C, Mansuroglu B, Unluer E. Primary squamous cell carcinoma of the ureter presenting with urinoma. A case report. Int Urol Nephrol. 1997;29(2):163-165.
doi pubmed - Ko HL, Tsang YW, Chi KH. Cutaneous metastases from squamous cell carcinoma of the ureter. Med Princ Pract. 2007;16(6):460-462.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.