Figures
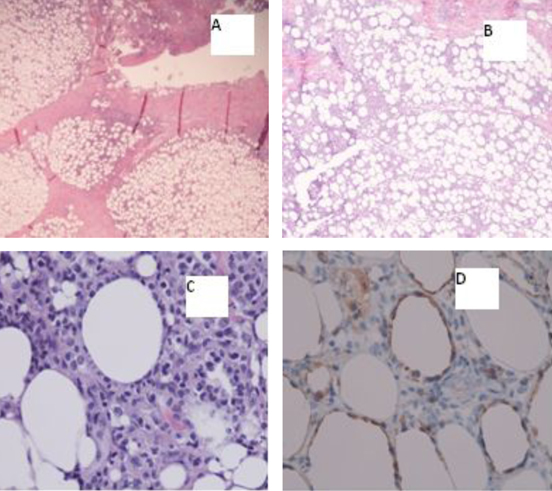
Figure 1. A) Inflammatory subcutaneous infiltrate with lobular pattern (20х); B) Inflammatory subcutaneous infiltrate with lobular pattern (40х); C) Atypical/neoplastic cells “rimming fat lobules” (400х); D) Cytotoxic immunohistochemical stain “perforin” labels the neoplastic cells, and again highlights the fat rimming (400х).
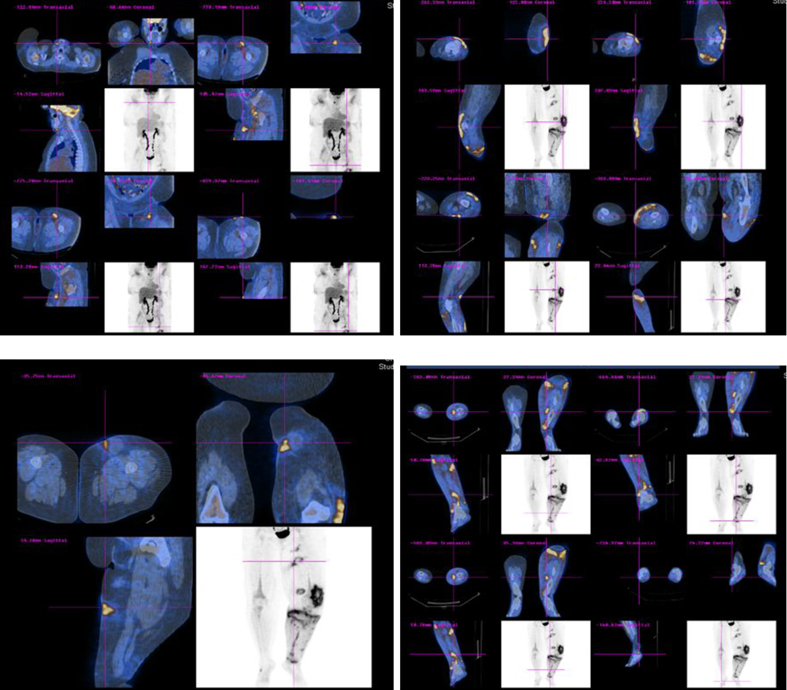
Figure 2. Whole body PET-CT scan showing multiple areas of hypermetabolic activity.
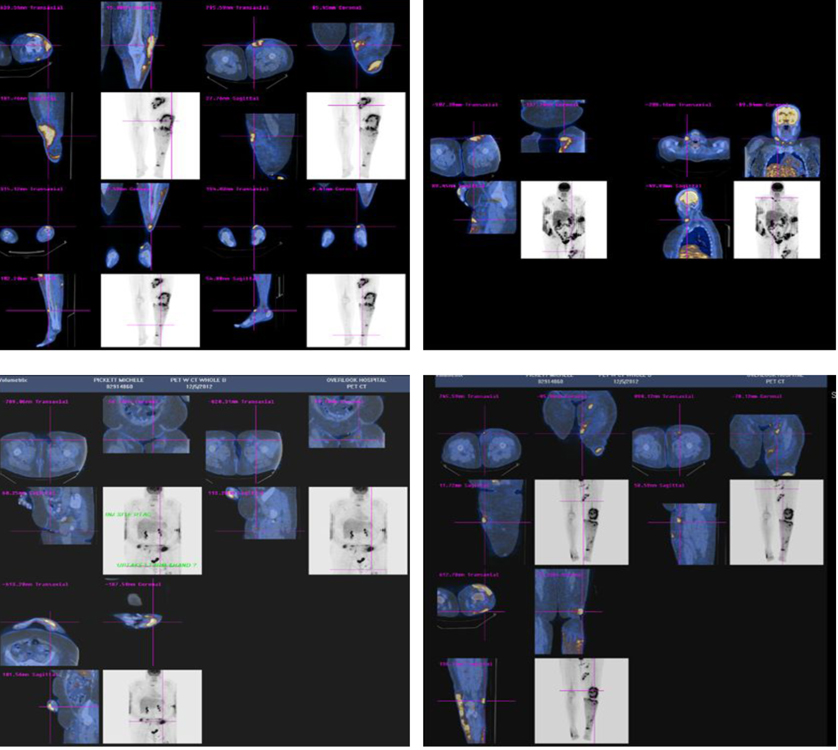
Figure 3. Whole body PET-CT scan showing worsening of lymphoma with increase hypermetabolic activity in lower extremities, submandibular region and abdomen.
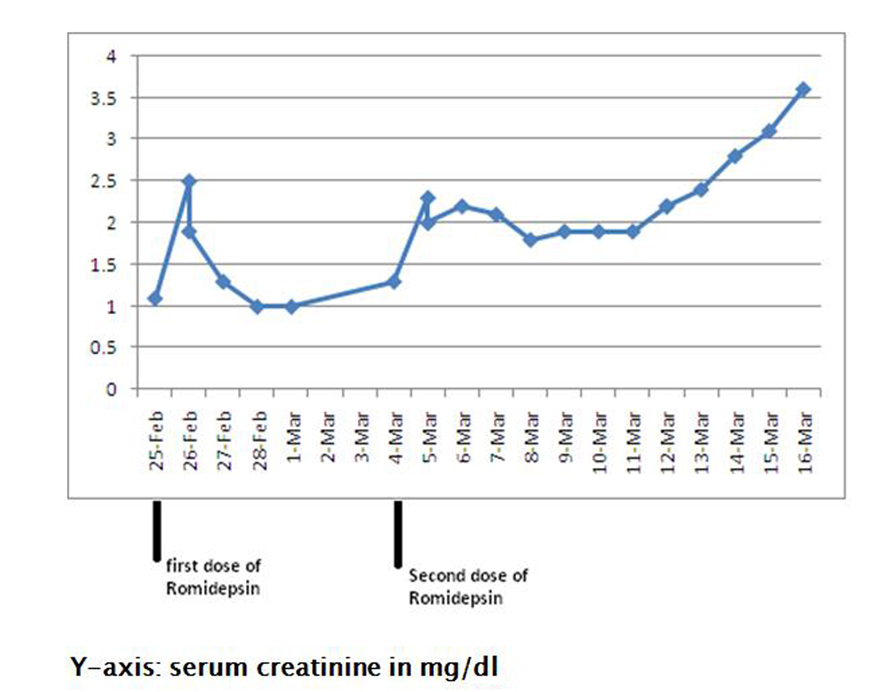
Figure 4. Showing rise in serum creatinine from 1.1 mg/dL (baseline) to 3.6 mg/dL following romidepsin therapy.
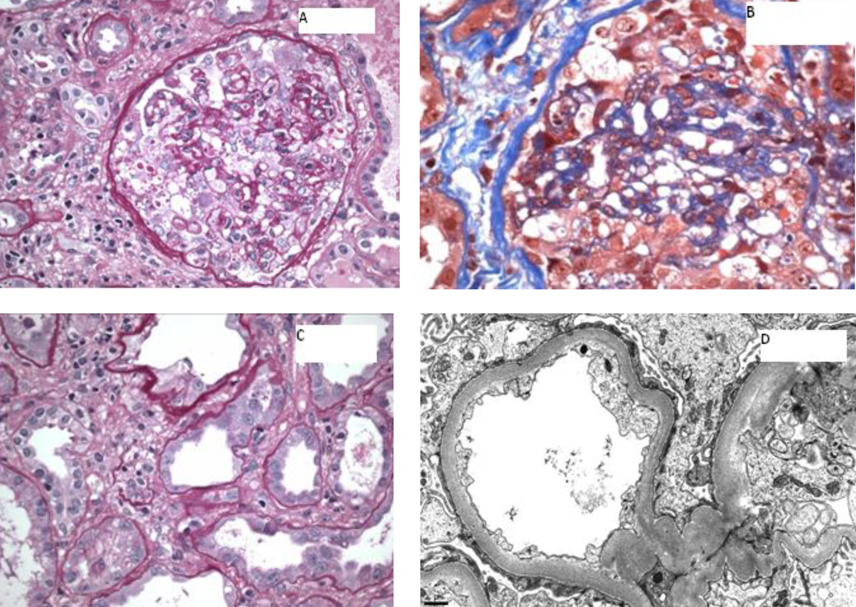
Figure 5. A) A glomerulus showing global implosive collapse of capillary lumina and prominent hyperplasia of epithelial cells, some of which contain prominent protein droplets (PAS stain; original magnification х 200); B) A glomerulus showing implosive collapse lumina and prominent hyperplasia of epithelial cells (Masson’s trichrome stain; original magnification х 400); C) Proximal tubules displaying loss of apical brush border and cytoplasmic attenuation (PAS stain, original magnification х 400); D) Electron photomicrograph showing diffuse foot process effacement (10,000 х).
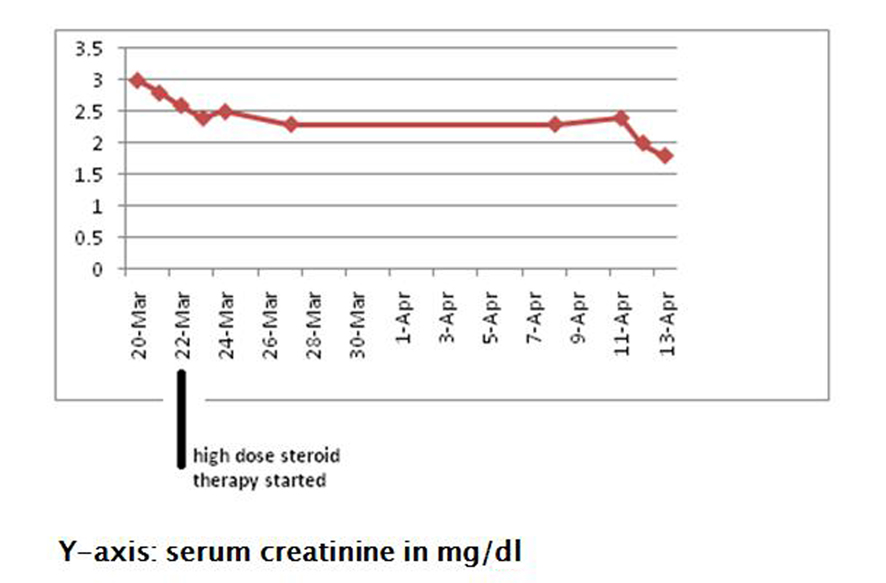
Figure 6. Showing improvement in serum creatinine following treatment with high dose steroids.