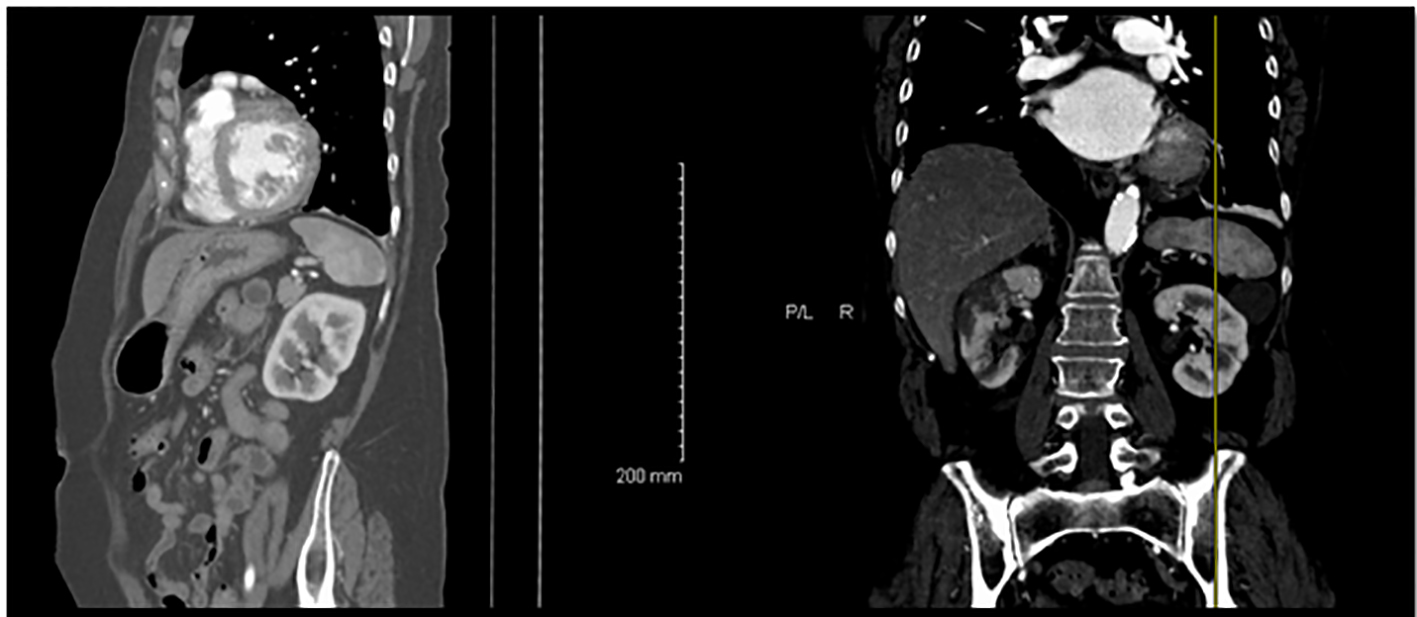
Figure 1. CT scan of the abdomen showing bilateral kidney infarctions.
| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 5, Number 1, March 2016, pages 11-15
Acute Renal Infarction Pathogenesis and Atrial Fibrillation: Case Report and Literature Review
Figures