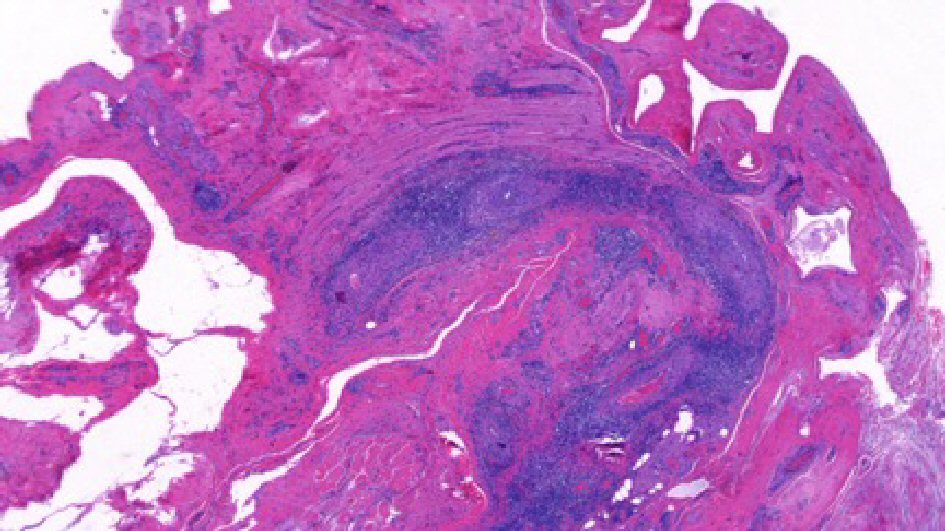
Figure 1. Left paratesticular tissue with perivascular infiltrates containing of lymphocytes and plasma cells (H&E, 20 × original magnification).
| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 7, Number 1, March 2018, pages 32-37
Minocycline-Induced Polyarteritis Nodosa Presenting With Testicular Pain: A Case Report and Selected Review of the Literature
Figures
Table
| Study, date | Patient age/final Dx | CC | Labs and ultrasound | Pathology | Tx | Sx after tx | Significance |
|---|---|---|---|---|---|---|---|
| ANA: anti-nuclear antibody; ANCA: anti-nuclear cytoplasmic antibody; Asymp-: asymptomatic; Avg: average; Bx: biopsy; CRP: C-reactive protein; C/W: consistent with; ESR: erythrocyte sedimentation rate; PAN: polyarteritis nodosa; Sx: symptoms; Tx: treatment; U/S: ultrasound. | |||||||
| Lenert, 2013 [3] | 21/minocycline-induced systemic PAN | Left testicular pain + systemic sx | Labs: elevated ESR, CRP, (+) p-ANCA, (+) ANA; U/S: wedge-shaped lesion | Medium-size testicular artery with mononuclear cell infiltration and area of testicular necrosis | Removal of minocycline, short course of prednisone and hydroxychloroquine | Asymp- and disease free at 2 years | Systemic vasculitis associated with chronic minocycline use |
| Gervaise, 2014 [4] | 28/systemic PAN | Right testicular pain | Labs: mildly elevated CRP; U/S: no Doppler flow in right testis with numerous hypoechogenic areas and some areas of normal parenchyma | Gross: heterogeneous in appearance with alternating areas of ischemia without necrosis and healthy parenchyma c/w acute vasculitis | IV prednisolone and cyclophosphamide | Asymp- | Diagnosis of testicular vasculitis on CT angio: thrombosis of distal testicular artery, no confirmed biopsy |
| Bing, 2012 [5] | 46/systemic PAN | Left flank pain with gross hematuria after running | Labs: elevated ESR and CRP, anemia, (-) ANA, (-) ANCA; renal U/S: left-sided, upper pole, pelvi-calyceal distension and peri-nephric edema | N/A | Glucocorticoid, cyclophosphamide, methotrexate | Asym- and disease free at 2 years | Diagnosis based on presence of aneurysms on left renal angiogram |
| Toepfer, 2011 [6] | 55/systemic PAN | Left testicular pain, with recurrence on the right 3 weeks after initial evaluation, recurrent systemic ischemic events | Labs: all (-); U/S: decreased blood flow | Testicular specimens: interstial hemorrhage and focal atrophy; Abdominal wall skin bx: thrombotic vasculopathy with leukocytoclastic vasculitis | Bilateral orchiectomy, methylprednisone + cyclophosphamide | Recurrence of ischemic events at 3 weeks and 5 weeks; asymp- after systemic tx at 6 months | Asynchronous testicular necrosis as initial sign of systemic PAN |
| Ahmad, 2010 [7] | 65/systemic PAN | Left testicular pain and swelling, developed frank painless hematuria during workup | Labs: (+) ANCA, elevated ESR; U/S: mycotic aneurysmal lesions of the testicle | N/A | Glucocorticoid | “Cinically well” | Left renal hematoma on CT scan, small aneurysms found in both kidneys on angiography |
| Meeuwissen, 2008 [8] | 72, 61, 28/systemic PAN | Testicular pain preceeding systemic symptoms (1), concurrent systemic sx and testicular pain (2) | Labs: elevated ESR, CRP, (-) ANCA, (-) ANA, anemia; U/S: heterogenic, enlarged testis | Gross: edematous, blue colored testis with multiple necrotic areas; Microscopic: segmental destruction of vessel wall of small and medium-sized arteries by mononuclear inflammatory infiltrate; fibrinoid necrosis and thrombi | Orchiectomy, methylprednisolone taper (after onset of systemic symptoms) | Asymp- and disease free at 16 months - 80 months | Testicular involvement as prominent sign of PAN |
| Kolar, 2007 [9] | 29/systemic PAN | Right scrotal pain + systemic sx | Labs: elevated ESR, CRP, (-) ANCA; U/S: enlarged and swollen right epididymis with reduced blood flow; reduced testicular artery flow | N/A | Glucocorticoids + cyclophosphamide | N/A | Improved testicular artery flow after systemic treatment without need for orchiectomy |
| Susanto, 2003 [10] | 74/systemic PAN | Left testicular pain + systemic sx | Labs: elevated ESR, CRP, anemia, leukocytosis, microscopic hematuria; (-) ANCA; U/S: small right testicular cyst and mild enlargement of left testicle with normal epididymis | Skin/muscle bx: vasculitis of medium vessels with mixed cellular infiltrate in intramuscular arterioles and their branches | Oral prednisone (1 mg/kg/day) and cyclophosphamide (2 mg/kg/day) × 6 months | Asymp- at 1 year | Febrile episode of epididymo-orchitis as initial manifestation of PAN |
| Eilber, 2001 [11] | 43/systemic PAN | Hematuria, left testicular mass, systemic sx | Labs: elevated ESR, (+) ANA; U/S: suspicious heterogeneous intratesticular lesion | Inflammatory infiltrate and thrombosis in vessel lumina, necrosis of intimal layer | Orchiectomy only | Asymp- | PAN presenting with hematuria and testicular lesion |
| Brimo, 2011 [12] | 35 (avg) 23-53 (range)/isolated testicular PAN (12), systemic PAN (2) | Testicular pain (86%), mass (7%) | Labs: all negative except 2 with elevated CRP and ESR, (-) ANCA; 1 with (+) ANA; U/S: hypoechoic mass suspicious for cancer | Transmural necrotizing inflammation of small to medium-sized ateries with fibrinoid necrosis and acute inflammation | Orchiectomy, systemic treatment: predisone, or prednisone + cytoxan (in half of isolated cases and all of systemic cases) | N/A | Case report of testicular vasculitis, 14 confirmed to be PAN, half of isolated cases still received systemic treatment |
| Fraenkel-Rubin, 2002 [13] | 26/iIsolated testicular PAN | Left testicular pain | Labs: negative ESR, CRP, ANA, ANCA, CBC; U/S: diffuse damage consistent with interstitial process | Fibrinoid necrosis of medium and small sized arteries with acute transmural inflammation with lymphoplasmacytic and eosinophilic infiltrates | Orchiectomy only | Asymp- and disease free at 2.5 years | Use of Birmingham Vasculitis Activity Score (BVAS) in determining need for systemic treatment for isolated PAN |
| Pastor-Navarro, 2007 [14] | 26/isolated testicular PAN | Painful bilateral testicular swelling | Labs: all (-); U/S: multiple non-vascularized, heterogeneous, hypoechoic focal lesions; small reactive hydrocele | Areas of intraparenchymal hemorrhage, fibrinoid necrosis, pleomorphic infiltration | Right orchiectomy, glucocorticoid | Asymp- at 1 year | Concurrent bilateral testicular involvement |
| Tanuma, 2003 [15] | 40/isolated testicular PAN | Left testicular pain, with recurrence on right 16 months after initial diagnosis | Labs: (+) ANA; U/S: avascularity of bilateral testes | Fibrinoid necrosis of small and medium sized arteries with severe inflammatory infiltrate and near obstruction of arterial lumen | Bilateral orchiectomy | Asymp- and disease free at 22 months | Recurrent testicular PAN |
| Mukamel, 1995 [16] | 28, 35/isolated testicular PAN | Right painful testicular swelling and mass | Labs: all (-); U/S: intratesticular hyper- and hypoechogenic areas (1); normal with hydrocele (1) | Intratesticular hemorrhage and fibrosis, segmental fibrinoid necrosis, thrombosis, and perivascular fibrosis of small arteries; some aneurysmal dilatation | Orchiectomy only | Asymp- and disease free at 2 - 3 years | Isolated testicular PAN |
| Warfield, 1994 [17] | 19/isolated testicular PAN | Left testicular pain and swelling with recurrence in right testicle 12 months later | Labs: elevated ESR and CRP, (-) ANCA; U/S: heterogeneous echo pattern including areas suggestive of cystic change | Gross: scattered areas of hemorrhage of lower pole of testis; Microscopic: patchy, necrotizing vasculitis affecting medium and small arteries; fibrinoid necrosis of walls and transmural infiltrate of PMNs and lymphocytes | Left orchiectomy + cyclophosphamide × 1month, azathioprine and oral prednisone with short-term increase after recurrence on right side, long-term low dose prednisolone | Recurrence of sx at 12 months; asymp- and disease free at 18 months | Recurrence of sx while on systemic therapy |
| Fleischmann, 2007 [18] | 21/isolated testicular PAN + metastatic mixed germ cell tumor | Left painful scrotal swelling | Labs: N/A; U/S: enlarged left epididymis and calcifications | Mixed germ cell tumor of left testis; circumferential, transmural fibrinoid necrosis, inflammatory infiltrates composed of neutrophils and monocytes in or around the walls of small to medium-sized arteries | Orchiectomy only | Asymp- and disease free at 2 years | Isolated PAN presenting with mixed germ cell tumor |