

| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 7, Number 2, June 2018, pages 53-55
Idiopathic Renal Infarct as a Rare Cause of Acute Abdominal Pain: A Case Report and Review of Literature
Yadav Pandeya, c, Krishna Prasad Joshia, Akshay Goela, Priya Priyambadab
aDepartment of Internal Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, USA
bDepartment of Family and Preventive Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, USA
cCorresponding Author: Yadav Pandey, Department of Internal Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, USA
Manuscript submitted April 2, 2018, accepted April 20, 2018
Short title: Idiopathic Renal Infarct
doi: https://doi.org/10.14740/wjnu338e
| Abstract | ▴Top |
Renal infarction is a very rare disease. Due to the non-specific clinical presentation, diagnosis is often missed or delayed. As the result, a prolonged period of ischemia and irreversible renal damage is common. The broad availability of high-quality computed tomography (CT) imaging has made it possible to identify the cases early and initiate prompt treatment. We report a case of renal infarction that presented with acute abdomen. A 56-year-old man with the medical history of hypertension and diabetes mellitus presented to emergency department with a complaint of sudden onset of severe right lower abdominal pain for 1 day. CT scan of abdomen with contrast showed the striated appearance of the right kidney with hypoperfusion and wedge-shaped hypodensities throughout the kidney. After an extensive workup, no apparent cause of renal infarct was found. Due to the absence of underlying cause of atrial fibrillation or hypercoagulable disorder, no anticoagulation was started and he was discharged home on aspirin. Although the incidence of renal infarction is uncommon, it should always be suspected in the patient presenting with flank pain with nausea, vomiting, and fever, especially in presence of risk factor like atrial fibrillation and elevation of lactose dehydrogenase (LDH) with normal or mildly elevated aminotransferases. Early diagnosis and management of renal infarction is important to prevent a prolonged period of ischemia and irreversible damage.
Keywords: Renal infarction; Flank pain
| Introduction | ▴Top |
Renal infarction is a very rare disease [1]. Due to the non-specific clinical presentation, diagnosis is often missed or delayed. As the result, prolonged period of ischemia and irreversible renal damage is common [2]. The broad availability of high-quality computed tomography (CT) imaging has made it possible to identify the cases early and initiate prompt treatment [3]. We report a case of renal infarction that presented with acute abdomen.
| Case Report | ▴Top |
A 56-year-old man with medical history of hypertension and diabetes mellitus presented to emergency department with complaint of sudden onset of severe right lower abdominal pain for 1 day. History was negative for urinary symptoms, constipation or diarrhea, trauma to abdomen or alcohol abuse. Three weeks prior, he was admitted in intensive care unit for suicidal attempt with acetaminophen overdose. History was negative for fever, chills, joint pain, rashes or kidney stones. Vital signs in emergency department showed BP 145/74, HR 87/min, RR 16/min, and temperature 36.3 °C. Systemic examination was positive for mild tenderness at right lower abdomen and severe tenderness at right costovertebral angle. Chest exam was normal, cardiovascular exam revealed systolic murmur at the mitral area and patient said he was told to have murmur in the past. Initial lab tests revealed WBC 16,650, Hb 14.4 g/dL, and platelet 432,000. Urinalysis showed WBC 6 - 10, RBC 3 - 5, negative leukocyte esterase and nitrite. Liver function showed ALT 77, AST 116, LD 1,051 with normal bilirubin, albumin and INR. Liver function was probably deranged from recovering liver injury from acetaminophen overdose but LD was disproportionately high. Urine drug screen was negative. CT scan of abdomen with contrast showed striated appearance of the right kidney with hypoperfusion and wedge-shaped hypodensities throughout the kidney (Figs. 1 and 2). Given radiographic appearance, acute onset, and evidence of leukocytosis, pyelonephritis versus multifocal infarction were suspected. He was started on antibiotics for pyelonephritis. But the clinical picture was more favorable for kidney infarction due to absence of fever, urinary symptoms and normal urinalysis. Urine culture showed mixed flora. Ultrasound with Doppler study showed relative decrease in blood flow within the right peripheral renal cortex compared to the left and the study was negative for renal artery stenosis. Lactate dehydrogenase was elevated to 1,051 at admission, peaked at 2,049 and decreased to 733 at the time of discharge. Due to disproportionate rise of lactate dehydrogenase, renal infarct was the more likely cause. Electrocardiogram showed normal sinus rhythm with no evidence of atrial fibrillation. The patient developed fever during hospital stay and blood culture was positive for methicillin sensitive Staphylococcus auricularis. Transthoracic echocardiogram was normal, but due to persistent fever, transesophageal echocardiogram was done that showed no vegetation and showed trivial mitral and tricuspid regurgitation with normal left ventricular ejection fraction.
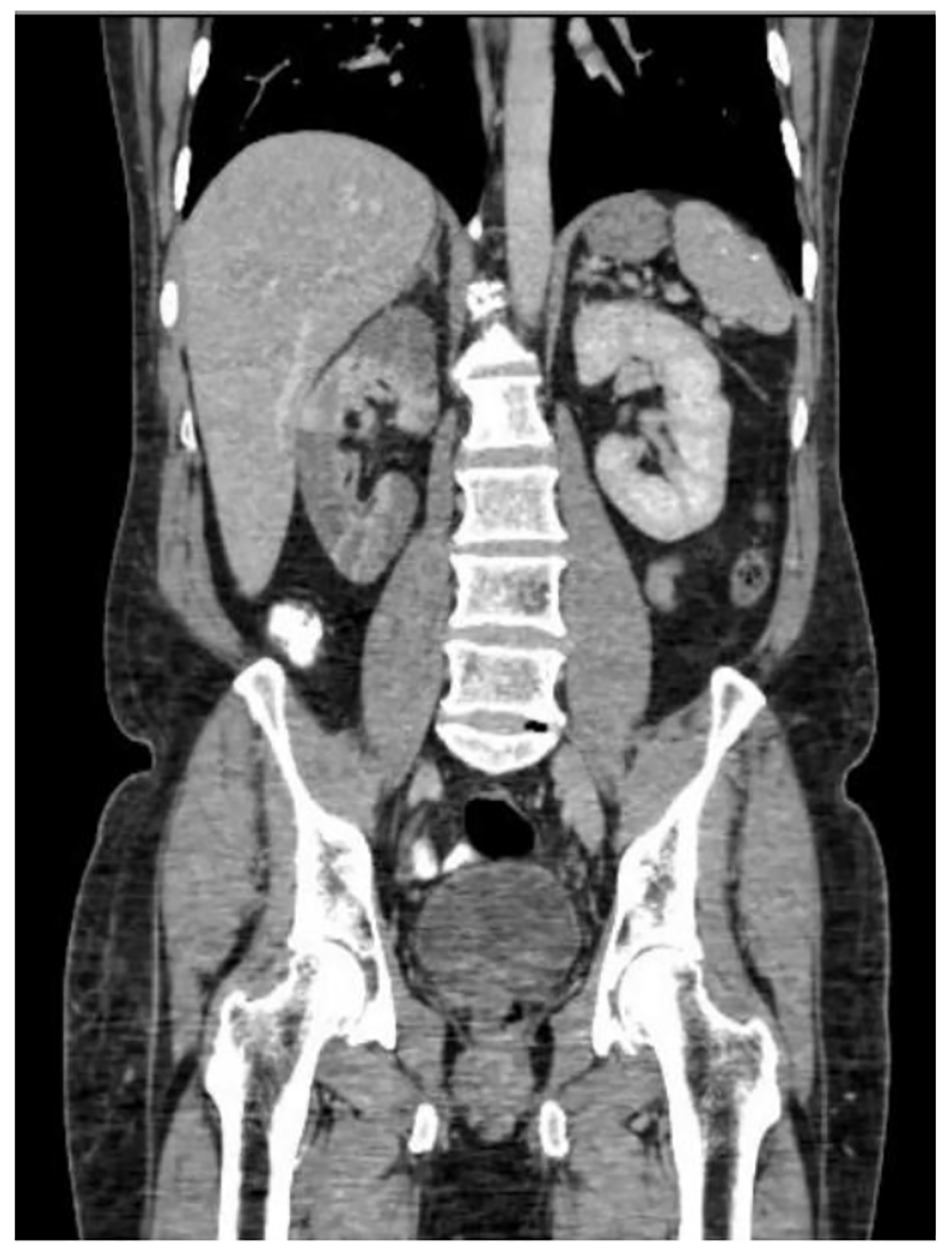 Click for large image | Figure 1. CT scan of abdomen showing renal infarction. |
 Click for large image | Figure 2. CT scan of abdomen (cross-section view). |
Lab tests were negative for antinuclear antibody, antinuclear cytoplasmic antibody, hepatitis B, hepatitis C and HIV. CT angiogram showed normal aorta, normal main renal arteries without evidence of dissection, luminal irregularity, or ostial stenosis (Figs. 3 and 4). Hypercoagulable study was negative for Lupus anticoagulant panel, antithrombin III deficiency, protein C and protein S deficiency and factor V Leiden mutation. After extensive workup, no apparent cause of renal infarct was found. Due to absence of underlying cause of atrial fibrillation or hypercoagulable disorder, no anticoagulation was started and he was discharged home on aspirin.
 Click for large image | Figure 3. CT angiogram anterior view. |
 Click for large image | Figure 4. CT angiogram posterior view. |
| Discussion | ▴Top |
Renal infarction is a rare cause of abdominal pain. In a study done in 1940, review of 14,411 autopsies reveled renal infarction in 205 patients, with incidence of 1.4% [4]. In another study, out of 250,000 patients seen in the emergency department, only 17 were diagnosed with acute renal infarction [5]. Although very few cases are reported, incidence of renal infarction is probably higher, as diagnosis is often missed or delayed as the presentation overlaps with other common conditions like nephrolithiasis and pyelonephritis [6]. Causes of renal infarction can be divided into cardiogenic thromboembolism originating in heart or aorta and in situ thrombosis. In a case series of 438 patients done over 20 years, cardiogenic origin was the most important cause of renal infarction accounting for 55% of cases with atrial fibrillation being the most common cause [7].
Patient with renal infarction presents with acute onset flank pain associated with nausea, vomiting and fever [2, 8]. Patient is often hypertensive at presentation because of activation of renin angiotensin-aldosterone system [2, 5]. Hematuria and proteinuria with elevation of serum creatinine is common in renal infarction [7]. Interestingly, elevation of lactose dehydrogenase (LDH) is very common in renal infarction. In clinically suspected patients, elevation of LDH with normal or mildly elevated aminotransferases is strongly suggestive of renal infarction [2, 3, 8]. As mentioned earlier, diagnosis of renal infarction is often delayed due to absence of classic symptoms on presentation. Contrast-enhanced CT is often diagnostic with feature of wedge-shaped perfusion defect [3, 9].
Treatment approach of renal infarction depends on time period of symptom onset to diagnosis, type and severity of renal artery occlusion, presence or absence of persistent hypertension and underlying disease. In presence of clear indication secondary to underlying disease like atrial fibrillation, left ventricular thrombus or any other hypercoagulable state, anticoagulation is beneficial but the role of prophylactic anticoagulation in the absence of a hypercoagulable state or an embolic source is less certain [2, 3, 5, 8]. Clinical judgement based severity of disease and presence of other co-morbidities is necessary in such cases. In our patient, we did not find any underlying cause needing anticoagulation. He was started on aspirin without anticoagulation due to absence of evidence of benefit of prophylactic anticoagulation.
Conclusion
Although the incidence of renal infarction is uncommon, it should always be suspected in patient presenting with flank pain with nausea, vomiting and fever, especially in presence of risk factor like atrial fibrillation and elevation of LDH with normal or mildly elevated aminotransferases. Early diagnosis and management of renal infarction is important to prevent prolonged period of ischemia and irreversible damage.
| References | ▴Top |
- Lopez VM, Glauser J. A case of renal artery thrombosis with renal infarction. J Emerg Trauma Shock. 2010;3(3):302.
doi pubmed - Bourgault M, Grimbert P, Verret C, Pourrat J, Herody M, Halimi JM, Karras A, et al. Acute renal infarction: a case series. Clin J Am Soc Nephrol. 2013;8(3):392-398.
doi pubmed - Hazanov N, Somin M, Attali M, Beilinson N, Thaler M, Mouallem M, Maor Y, et al. Acute renal embolism. Forty-four cases of renal infarction in patients with atrial fibrillation. Medicine (Baltimore). 2004;83(5):292-299.
doi - HJ H, CB C. Renal infarction: Statistical study of two hundred and five cases and detailed report of an unusual case. Arch Intern Med [Internet]. 1940;65(3):587-594.
doi - Paris B, Bobrie G, Rossignol P, Le Coz S, Chedid A, Plouin PF. Blood pressure and renal outcomes in patients with kidney infarction and hypertension. J Hypertens. 2006;24(8):1649-1654.
doi pubmed - Lessman RK, Johnson SF, Coburn JW, Kaufman JJ. Renal artery embolism: clinical features and long-term follow-up of 17 cases. Ann Intern Med. 1978;89(4):477-482.
doi pubmed - Oh YK, Yang CW, Kim YL, Kang SW, Park CW, Kim YS, Lee EY, et al. Clinical characteristics and outcomes of renal infarction. Am J Kidney Dis. 2016;67(2):243-250.
doi pubmed - Domanovits H, Paulis M, Nikfardjam M, Meron G, Kurkciyan I, Bankier AA, Laggner AN. Acute renal infarction. Clinical characteristics of 17 patients. Medicine (Baltimore). 1999;78(6):386-394.
doi - Priyambada P, Joshi KP, Azhar G. An unusual cause of right lower abdominal pain in young female: A case report and review of literature. Case Reports Intern Med [Internet]. 2016;3(1):63-66.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.