

| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 2, Number 2, November 2013, pages 76-78
Wilms’ Tumor With Transureteric Extension Into Bladder
Bhanu Mariyappaa, b, Japinder Khosaa, Andrew Barkera, Naeem Samnakaya
aDepartment of Surgery, Princess Margaret Hospital for Children, Perth, Western Australia, Australia
bCorresponding author: Bhanu Mariyappa, Department of Paediatric Surgery, Princess Margaret Hospital, Perth, Western Australia, Australia
Manuscript accepted for publication September 25, 2013
Short title: Wilms’ Tumor
doi: https://doi.org/10.4021/wjnu84w
| Abstract | ▴Top |
We report a case of 15 months old boy with Wilms’ tumor with transureteric extension of the tumor into the bladder. His chief complaint was passage of brownish yellow pasty like material per urethrally. Examination revealed a mass in the right flank. CT scan showed a large mass arising from the right kidney and extending down the right dilated ureter into the bladder. A radical right nephroureterectomy was performed. Histopathology revealed triphasic nephroblastoma without invasion of ureteric wall or nodal metastasis. The tumor was classified as Cassady stage 1 Wilms’ tumor and hence did not require adjuvant chemotherapy or radiotherapy. If clinically suspicious of ureteric extension of tumor and if imaging does not pick it or is unclear, cystoscopy and retrograde pyelogram are recommended to prevent transecting unsuspected tumor in ureter which will upstage the tumor.
Keywords: Wilms’ tumor; Transureteric extension; Hematuria
| Introduction | ▴Top |
We report an interesting case of Wilms’ tumor with extension of the tumor in a polypoid fashion, through the ureter into the bladder.
It is very uncommon for Wilms’ tumor to extend into the ureter and bladder. According to the NWTSG database, ureteral extension is seen in only 2% of Wilms’ patients and bladder extension in even fewer [1]. Presence of gross hematuria suggests the possibility of involvement of the collecting system. Routine preoperative imaging with ultrasound and CT may detect such ureteric extension, so that the tumor and ureteral extension can be planned to be removed en bloc to avoid cutting across the tumor.
We outline the presentation, imaging, and management of our case of Wilms’ with ureteral extension in this article, as well as a review of the literature on the subject.
| Case Report | ▴Top |
A 15-month-old boy presented with a few days’ history of per urethral passage of brownish yellow pasty material, with straining and pain during micturition. There was no history of macroscopic hematuria. The child had a previous similar episode about 3 months prior which quickly settled down; hence his parents did not seek any medical attention.
Physical examination revealed a happy and active child with a firm, large, and non-tender lobulated mass in the right flank. Urinalysis revealed microscopic hematuria. Blood tests showed a hemoglobin of 90 g/L, normal calcium levels, normal liver function, and renal function. Serum LDH was elevated at 1,260 U/L. Urinary catecholamines were not elevated. The tumor markers NSE, AFP, and BHCG were not elevated. The coagulation screen was normal.
Ultrasound scan (USS) showed a large solid/cystic mass arising from the right renal bed. However, USS did not show ureteric extension. CT scan revealed an unusual multiloculated cystic/solid tumor replacing almost all of the right renal parenchyma and extending down the dilated, tortuous right ureter to the level of vesicoureteric junction (Fig. 1). There was no evidence of metastasis or extension of the tumor into the renal vein or venacava.
 Click for large image | Figure 1. CT scan showing tumor extending into bladder. |
Cystoscopy prior to excision showed the tumor protruding into the bladder in a polypoid fashion and did not seem to be invading the ureteric orifice or adjacent bladder wall macroscopically (Fig. 2). Cystoscopic biopsy of the protruding mass showed necrotic tissue with dystrophic calcium. A right radical nephroureterectomy was performed through flank and Pfannenstiel’s incision. A cuff of bladder wall was removed around the ureteric orifice, mainly to provide a margin of clearance in case the tumor was invading the ureteric wall.
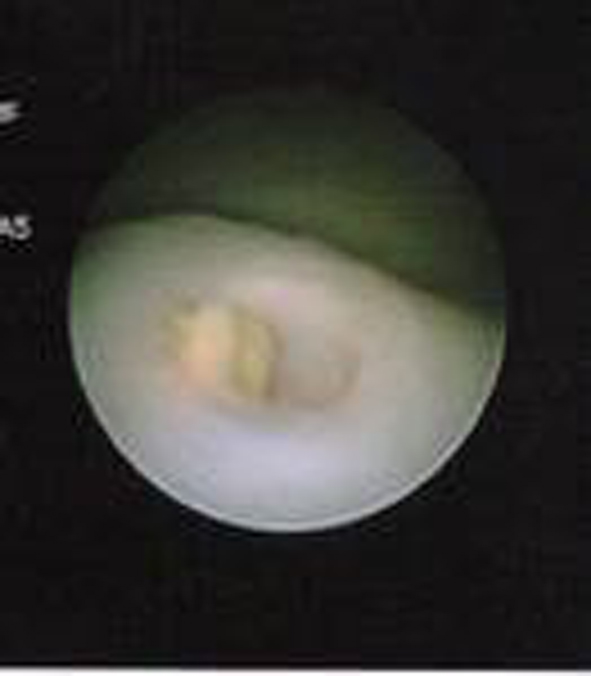 Click for large image | Figure 2. Cystoscopic view of tumor protruding into bladder. |
The tumor weighed 393 g. Macroscopically heterogenous tumor occupied the entire specimen with only a very fine outer rim of renal parenchyma evident at the lower pole. The tumor filled the pelvicalyceal system, with a large component prolapsing into the ureter. Microscopically this was a triphasic Wilms’ tumor with favorable histology, without sinus, capsular or lymph node involvement and hence the designation was stage 1 tumor (by Cassady criteria - under 24 months of age, unilateral, favorable histology, no metastases). The patient hence did not receive adjuvant chemotherapy or radiotherapy. Follow-up imaging 12 months post surgery did not show any recurrent disease.
| Discussion | ▴Top |
Wilms’ tumor typically presents as an intrarenal mass which invades and distorts renal parenchyma. The tumor may extend beyond the renal capsule, invade the renal sinus, and metastasize to regional lymph nodes or distant sites. It is very uncommon for the Wilms’ tumor to extend into the ureter and bladder. NWTSG database has identified only 45 patients (or 2% of their Wilms’ database) with ureteral extension; and only 7 of the 45 extended all the way into the bladder [1]. The mechanism of urothelial spread is thought to be caused by exfoliation of the tumor cells and implantation along the path of urine flow [2].
A typical intrarenal Wilms’ tumor presents with microscopic hematuria in only about 25% cases, whereas those with ureteric extension can have hematuria in 88% cases [3]. In the NWTSG database, gross hematuria was seen in 49% of cases of Wilms’ tumor with ureteric involvement [1]. Hence the symptom of gross hematuria should raise the suspicion of tumor extending into the collecting system. Passage of tumor per urethra occurs due to dislodged fragment of necrotic tumor tissue [4]. As in our case, it should raise suspicion of tumor extension into the ureter or bladder. Preoperative imaging may not detect ureteral extension of the tumor in all cases. In the NWTSG database, only 14 of 45 patients (32.1%) had ureteral extension identified by preoperative imaging. CT scan alone identified ureteral extension of Wilms’ in 10 patients [1].
It is very important to be aware of ureteric extension of the tumor preoperatively, so that the surgeon will not cut across the tumor in the ureter, producing local spillage of the tumor and leaving residual tumor in the distal ureter contributing to upgrading of the tumor to stage 3. If the ureteral extension is entirely removed intact, with no other tumor spread, the patient would be considered to have a stage 2 tumor (unless it meets Cassady criteria for a stage 1, as our case did).
Any child with Wilms’ tumor and gross hematuria, hydronephrosis or a non-functioning kidney should alert the surgeon to the possibility of ureteral extension. If not detected on preoperative ultrasound or CT, but is clinically suspected, a cystoscopy and retrograde pyelogram would help.
Presence of intralobar nephrogenic rests in the histological examination calls for closer look at the resected margin of ureter because nearly 50% of those children with ureteral extension had intralobar nephrogenic rests in NWTSG database [1].
Mere extension of the tumor into the ureter or bladder without actual invasion of the wall does not upstage the tumor [3]. It is important to be aware of this so that overstaging of the tumor and associated morbidity of the adjuvant treatment can be avoided. Johnson et al have suggested the need for cystoscopic surveillance post operatively to detect tumor recurrence [5]; however, NWTSG database analysis does not support such a recommendation because local recurrence after complete resection has not been documented.
Conclusions
Ureteral extension in Wilms’ tumor is very rare and accounts for 2% of cases, with bladder extension seen in even fewer cases. Ureteral and bladder extension should be suspected in patients with gross hematuria, tumorurea, hydronephrosis or non-functioning kidney. If ureteral extension is clinically suspected but not picked up on preoperative CT or ultrasound, cystoscopy with retrograde pyelogram should be considered. Recognition of ureteral and bladder involvement is important to carry out complete resection without spillage. The prognosis of these children with complete resection remains good. There is no need for routine cystoscopic surveillance to monitor for intravesical recurrence, as there has not been a reported case with intravesical recurrence.
| References | ▴Top |
- Ritchey M, Daley S, Shamberger RC, Ehrlich P, Hamilton T, Haase G, Sawin R. Ureteral extension in Wilms' tumor: a report from the National Wilms' Tumor Study Group (NWTSG). J Pediatr Surg. 2008;43(9):1625-1629.
doi pubmed - Stevens PS, Eckstein HB. Ureteral metastasis from Wilms tumor. J Urol. 1976;115(4):467-468.
pubmed - Mitchell CS, Yeo TA. Noninvasive botryoid extension of Wilms' tumor into the bladder. Pediatr Radiol. 1997;27(10):818-820.
doi - Wicklund RA, Tank ES. Polypoid renal pelvic lesions in children. J Urol. 1980;123(6):943-944.
pubmed - Johnson F, Luttenton C, Limbert D. Extrarenal and urothelial Wilms tumor. Urology. 1980;15(4):370-373.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.